Alternative names for female infertility
Sterility; Subfertility; Female factor infertility
What is infertility in women?

Fertility test. Male and female home-use Fertell fertility test kit. At bottom right is the wand used to test female fertility. It measures the amount of follicle stimulating hormone in the woman's urine which is an indicator of ovarian reserve (how many eggs are left in the ovaries).
Infertility is when a couple are unable to conceive a child after 12 months of regular intercourse without the use of contraception. Most couples (approximately 9 in 10 couples) will conceive after 1 year of trying, although some couples may need a longer duration to conceive. Therefore, the term ‘subfertility’, which suggests a reduced chance of conception, is preferred by many practitioners to ‘infertility’, which implies an absolute inability to conceive.
Some conditions that affect fertility signify a very low chance of conception, for example, the absence of sperm in a man, or if both fallopian tubes have been removed in the woman. Thus, it is possible to identify the likely reason for subfertility in some couples as being either due to a reason in the female or male partner (described as ‘female factor infertility’ or ‘male factor infertility’). However, in a significant proportion of couples (over one third), there are reasons for subfertility present in both partners, and conversely some causes of subfertility are not easy to identify even after investigation called ‘unexplained infertility’. Thus, it is not always accurate (or fair) to attribute subfertility to just one partner, as there may be unidentified issues affecting the other partner. The purpose of investigation is to identify medical issues that can be resolved by treatment, rather than to assign blame (which is not helpful), in order to maximise the chance of pregnancy.
Infertility can be a distressing and emotional issue for both women and men and it is important that professional advice and counselling is offered for affected couples. Some causes of infertility in women are treatable e.g. with assisted conception (eg with in vitro fertilisation (IVF) treatment) and for those that are not, sperm / egg donation, surrogacy, adoption, can represent alternative avenues for starting a family.
What causes infertility in women?
There are a number of causes of infertility in women (including problems affecting 1. ovulation, 2. the fallopian tubes, or 3. the womb), but sometimes despite investigation the cause remains unknown and may be termed ‘unexplained infertility’.
The most common reasons why a woman may not be able to conceive a child include:
- Decreased Ovulation: Infrequent release of an egg from the ovary during each menstrual cycle. The commonest causes are Polycystic Ovary Syndrome (PCOS), hypothalamic amenorrhoea (insufficient energy available for fertility), hyperprolactinaemia, and Premature Ovarian Insufficiency(early menopause occurring before the age of 40yrs).
- Blockage of one or both fallopian tubes can be referred to as ‘tubal infertility’. This can be due to previous infections causing ‘Pelvic Inflammatory Disease’ (PID); the most common infection leading to inflammation and blockage of the fallopian tubes is Chlamydia, which is a sexually transmitted disease. Ectopic pregnancy can sometimes need treatment involving the removal of a fallopian tube on the affected side; if both tubes are removed after treatment of more than one ectopic pregnancy, this can result in tubal infertility. Pelvic adhesions (fibrous strands that can occur due to inflammation after surgery, or through inflammation in the abdomen e.g. appendicitis, inflammatory bowel disease) can also lead to blockage of the fallopian tubes.
- Problems affecting the womb (uterus), such as fibroidsand endometriosis. Fibroids are benign non-cancerous tumours of muscle and fibrous tissue that can prevent implantation of the embryo into the womb (especially those that sit or project inside the womb cavity). Fibroids can be treated with medicines and / or removed with surgery. Endometriosis is where tissue usually only present in the lining of the womb (endometrium) may be found in other areas of the body such as the fallopian tubes, which can lead to infertility. Rarely, women who have had surgery in the womb for example to remove the remnants of a pregnancy after miscarriage may develop scarring of the womb (Asherman’s syndrome), and have a reduced chance of implantation of an embryo.
Other factors to consider for safeguarding reproductive health include avoidance of stress, maintenance of a healthy body weight, avoidance of smoking or illicit drugs, limiting alcohol use, checking for normal thyroid function, and taking folic acid (vitamin B9) (check with your doctor for information regarding how much to take as some women may need higher doses). It is possible, that the cause of infertility remains ‘unexplained’ even after investigation.
What are the signs and symptoms of infertility in women?
Some signs and symptoms may hint to the underlying cause of infertility.
Women having regular menstrual cycles (periods), usually indicates that they are ovulating regularly (i.e. an egg is released from the ovary each month). Conversely, women who are not ovulating regularly may have infrequent periods (termed oligomenorrhoea), or absent periods (termed amenorrhoea). A high progesterone level taken midway through the latter half of the menstrual cycle i.e. mid-luteal phase e.g. day 21 of a 28 day cycle, can be used to confirm ovulation.
Polycystic ovary syndrome (PCOS) is the most common cause of not ovulating regularly, which can present as irregular periods. Women with PCOS may have higher levels of androgens, which can manifest as excess hair growth on the face and body, or hair loss from the scalp in a male pattern (alopecia). The second commonest cause of infrequent ovulation and absent periods (amenorrhoea) is called ‘hypothalamic amenorrhoea’, which is due to a combination of low body weight, excessive exercise, and psychological stress, often on a background of genetic predisposition. Thus, a low body weight, or a history of weight loss, or heavy exercise schedule, could indicate hypothalamic amenorrhoea as a possible cause.
Women with endometriosis or fibroids may have painful (dysmenorrhoea) or heavy (menorrhagia) periods, lower abdominal pain, or painful sexual intercourse (dyspareunia).
How common is infertility in women?
Infertility occurs in 1 in 7 couples. Infertility is more common as the female partner increases in age and approaches the menopause. Likewise, the response to fertility treatments is not as successful in women as they approach the menopause. Consequently, from a fertility point of view, it is a good idea to try to start a family at a younger adult age, if possible.
Is infertility in women inherited?
Many conditions that can cause infertility, such as polycystic ovary syndrome (PCOS), endometriosis, hypothalamic amenorrhoea, and premature ovarian insufficiency (POI), often occur more frequently in members of the same family.
How is infertility in women diagnosed?
The main approach is to investigate whether ovulation is happening regularly, whether there are blockages to the fallopian tubes, or any issues affecting the womb.
Blood tests are usually carried out within the first five days from the start of a woman’s period (termed early follicular phase) to assess hormone levels. These tests, such as a follicle stimulating hormone (FSH) level, provide an approximate measure of ‘ovarian reserve’ – that is, the number of eggs a woman has left in her ovaries. If the function of the ovaries is starting to decrease with increasing age, the FSH level will be increased. Increasingly in many hospitals, a test to measure anti-Müllerian hormone in the blood can be used as a more accurate measure of ovarian reserve. An ultrasound scan to count the number of follicles in the ovary during the first few days of a period (antral follicle count) is also another method of estimating the ovarian reserve. These tests can estimate how likely the ovaries are to be able to respond to hormonal stimulation with follicle stimulating hormone (FSH)-like medications during assisted reproduction. A blood test for progesterone level can be taken on day 21 of the menstrual cycle to confirm that eggs are being released from the ovary (ovulation).
Tests for current or previous Chlamydial infection are carried out in blood, urine samples or genital swabs. A blood test is also usually taken to ensure that the woman has developed protection against rubella infection (previously known as ‘German measles’) as part of the initial fertility tests in case a pregnancy occurs as this can be harmful to the baby. Most women will have been immunised against rubella in the childhood immunisation programme.
To find out if the fallopian tubes are blocked or not and if the womb looks normal, one or two of the following tests can be performed:
- Hysterosalpingogram (HSG)- an X-ray of the pelvis, which is taken while injecting a dye through the neck of the womb to find out if the fallopian tubes are blocked or not.
- Hysterosalpingo Contrast Sonography (HyCoSy)- an ultrasound scan of the pelvis while injecting the bubbled water as a contrast to find out if the fallopian tubes are blocked or not.
- Laparoscopy- a keyholesurgical operation to allow the specialist to directly see the pelvis and fallopian tubes. This operation is combined with dye to check the fallopian tubes, called a laparoscopy and dye test.
- Hysteroscopy- an examination of the womb cavity with a camera to identify any problems within the womb.
What treatments are available?
It is important to advise the woman to try to be in the best possible health to conceive. This includes maintaining an ideal body weight (ideally a BMI over 19 and less than 25 kg/m2); taking regular exercise; avoidance of smoking; and limiting alcohol intake to two to three units per week.
More specific treatment will depend on the cause of infertility. In certain conditions such as high prolactin levels in the blood (hyperprolactinaemia), correction of the hormonal imbalance can restore ovulation.
In women with polycystic ovary syndrome (PCOS) who are overweight, weight loss (even a small amount) can help restore ovulation; other medications such as metformin can help reduce insulin resistance and restore ovulation. Ovulation can also be restored (ovulation induction) using the oral medications letrozole or clomiphene citrate, or by taking a medication containing follicle stimulating hormone (FSH) given by injection. During these treatments, women have to be carefully monitored to ensure that the ovaries do not become overly stimulated, or have more than one egg being released (which can lead to multiple pregnancy and cause additional health risks for mother and baby). For some selected women, an operation called ovarian diathermy (also known as ‘ovarian drilling’), whereby a few tiny punctures are made in the ovary using a laparoscope, can help to restore ovulation.
Specific treatment of other causes of infertility, such as removal or treatment of endometriosis, uterine fibroids, or uterine polyps, or pelvic adhesions, can help to improve fertility.
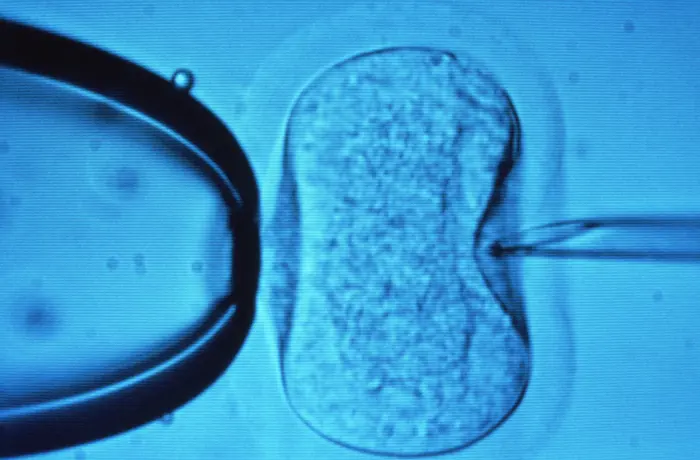
A light microscope image showing the process of in vitro fertilisation (IVF). A needle (right) is being used to inject a sperm cell directly into a human egg (centre). A pipette (left) is used to hold the egg steady while the needle is inserted.
For women with ovulatory infertility, tubal infertility, unexplained infertility, or even with multiple causes of infertility, including a problem in the male partner’s sperm, assisted reproduction techniques such as in vitro fertilisation (IVF) can be beneficial. IVF treatment involves stimulating growth of follicles in the ovary (which each contain an egg), collecting the eggs from a woman during a small operation, and then artificially fertilising them in the laboratory using the partner’s sperm. If fertilisation is successful and an embryo is formed, it is then transferred back into the woman’s uterus where, hopefully, it will implant and result in pregnancy.
The success of IVF treatment depends heavily on age; younger women have a higher pregnancy rate. Older women with very poor ovarian reserves, such as women with premature ovarian insufficiency, can choose to use donor eggs for assisted reproduction.
Another option, which may be recommended for patients without a womb (either following a hysterectomy (surgical removal of womb), or if the woman is born without a womb), is using a surrogate. In this case, assisted reproduction is carried out using the patient’s own eggs with the embryo then being implanted into the surrogate woman who carries the child until birth.
Are there any side-effects to these treatments?
In assisted reproduction, women are given medications called gonadotrophins (predominantly FSH) to stimulate the ovaries to produce eggs, which are then fertilised in a laboratory. A potential side-effect to this stimulation of the ovaries with FSH is the ‘ovarian hyperstimulation syndrome’ (OHSS). In OHSS, the ovaries become enlarged and fluid leaks into the abdomen (ascites), such that the patient may experience pain and swelling in the abdomen, and this may be accompanied by nausea, vomiting. In most cases, ovarian hyperstimulation syndrome resolves with time, but sometimes additional treatments like drainage of intra-abdominal fluid are required.
Couples who require investigation and treatment for fertility problems can find it emotionally stressful. Those in need of IVF may need more than one treatment cycle to achieve a pregnancy and each treatment cycle may last up to 6-8 weeks. In addition, donor egg or surrogacy treatments come with a large number of social and psychological implications such that fertility counselling is considered beneficial prior to such treatments.
What are the longer-term implications of female infertility?
Infertility can have significant impact on the mental health of both the woman and her partner, the impact on their relationship and on long-term wellbeing. When infertility is diagnosed, specialist counselling can help the couple better manage the implications of infertility and if fertility treatments are unsuccessful.
Other options for starting a family may also be considered such as sperm / egg donation, adopting or fostering a child.