Alternative names for Turner syndrome
Turner’s syndrome; Ullrich-Turner syndrome; gonadal dysgenesis
What is Turner syndrome?
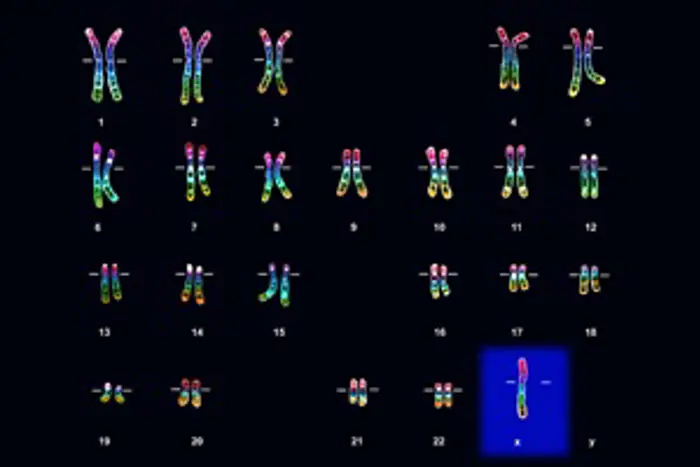
Light micrograph of the chromosomes (karyotype) of a female with Turner syndrome. Turner syndrome is caused by the presence of only one X chromosome (at bottom right, blue highlight).
Turner syndrome is a genetic disorder due to having only one of the usual two female X sex chromosomes (XO rather than XX). Chromosomes contain a detailed plan of our genetics, inherited from both parents and each cell in our body has 23 pairs. One pair is the sex chromosomes and determines the baby’s sex – usually, boys have an X and a Y chromosome (XY), whilst girls have two X chromosomes (XX).
An abnormality in one of the two X chromosomes in girls causes Turner syndrome. In around 50% of cases there is an entire X chromosome missing (see figure), or parts of the chromosome may be missing or rearranged. Sometimes the X chromosome is missing from only some cells. This is known as mosaicism and girls may show only mild features of Turner syndrome, depending on how many of the cells are affected.
What causes Turner syndrome?
The cause is unknown, but it occurs very early in foetal life.
What are the signs and symptoms of Turner syndrome?
Although many signs and symptoms are described in Turner syndrome, these vary widely between individuals. Often the diagnosis is only made during investigations for short stature or delayed puberty.
In infancy, girls with Turner syndrome can have puffy hands and feet (lymphoedema). Other features include short ‘webbed’ neck, low hairline, a high arched palate, widely spaced nipples and a ‘shield-like’ chest appearance. There can also be an increased number of moles and abnormal fingernails, which can be smaller than usual, or be ‘over-curved’.
The most serious problems involve the heart, such as narrowing of the main artery from the heart (aorta), known as coarctation, and some heart valve defects. There may also be dilation of the root of the aorta, which can rarely lead to a serious rupture or tear in the aorta (aortic dissection). There can be defects in the kidneys such as a ‘horseshoe’ kidney, where the two kidneys fuse together early on during development of the embryo, and appear horseshoe-shaped.
Repeated ear infections and glue ear are very common, as are minor vision problems including squints, drooping eyelid (ptosis), and colour blindness. Learning difficulties are not a feature of Turner syndrome although problems with non-verbal skills are common. Affected girls are on average 20 cm (eight inches) shorter than expected. Small size may be apparent from birth or in the first years of life.
Although ovaries are present at birth, these soon begin to fail, leading to ‘streak ovaries’. This causes underproduction of the female hormone oestrogen required for puberty, and also failure to produce mature eggs, leading to infertility. A long-term lack of oestrogen may lead to brittle bones (osteoporosis).
How common is Turner syndrome?
Turner syndrome only affects girls. It is a genetic condition and is therefore present at birth. Although Turner syndrome affects 1 in 30 female foetuses conceived, there is a very high miscarriage rate of affected pregnancies and Turner syndrome is found in 1 in 2,500 of live-born girls.
Is Turner syndrome inherited?
In the vast majority of girls, there are no other affected family members. One of each chromosome pair comes from either parent and in 80% of cases, the missing X-chromosome comes from the father.
How is Turner syndrome diagnosed?
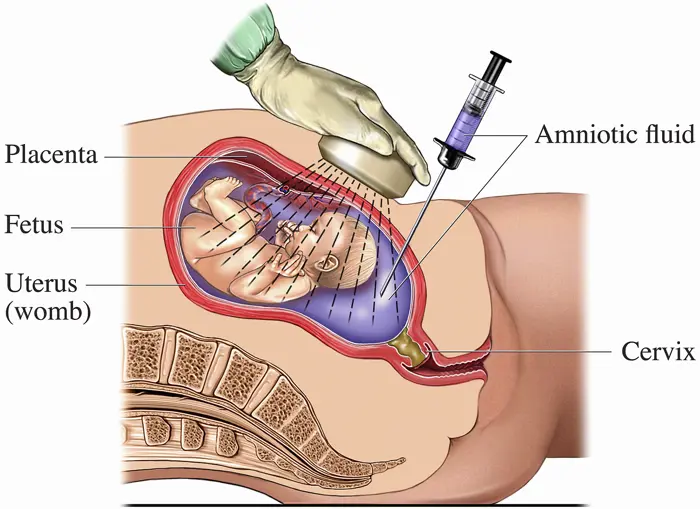
A medical drawing to show the process of amniocentesis, which can be carried out during pregnancy. A fine needed is used to take a sample of amniotic fluid from the mother's uterus (womb), which is then analysed to determine the karyotype (chromosome arrangement) of the fetus.
The diagnosis of Turner syndrome is made by chromosomal analysis or karyotyping, and involves a blood test.
Karyotyping can also be performed during pregnancy if there are significant concerns. This is done by analysing the fluid surrounding the foetus called amniocentesis. This is done after 13 weeks’ gestation. Associated complications are screened for at diagnosis and then from time to time afterwards as an outpatient. Testing can also be done through chorionic villus sampling.
As well as being diagnosed during pregnancy, Turner syndrome can be diagnosed shortly after birth, in childhood when growth is faltering, or during adolescence if the girl fails to enter puberty.
How is Turner syndrome treated?
Treatment of Turner syndrome depends on the symptoms the child shows. Health professionals from different specialities deal with any disorders of the heart, kidney, ears and eyes. Some physical features of Turner syndrome are purely cosmetic and do not need treatment. Psychological support may assist with educational or social difficulties.
Endocrinologists are involved in three main areas:
- Growth – most girls require a daily injection of growth hormone, which improves final height by an average of 7.5 cm (three inches). This is usually given from diagnosis or within the first years of life and continues until final height is achieved. Girls who benefit most from this treatment are those who start growth hormone early or are very short to begin with. The results of growth hormone treatment can vary with some girls benefitting more than others. Often a mild anabolic steroid called oxandrolone (taken by mouth) is added in from ten years of age to promote the effect of growth hormone.
- Puberty – absent puberty is very common in girls with Turner syndrome. Treatment involves the female hormone oestrogen with gradually increasing doses over several years, given by mouth from 12 or 14 years of age. This helps with breast development and maturation of the uterus, leading to the onset of periods. Once periods have started, they are usually maintained by hormone replacement of oestrogen and progesterone, using either the oral contraceptive pill or hormone replacement therapy.
- Fertility – because streak ovaries do not produce eggs, many women with Turner syndrome are infertile and require not only hormone therapy, but also egg donation and IVF treatment if they wish to fall pregnant. This is carried out through a specialist fertility Women with Turner syndrome who becomes pregnant requires close monitoring of their heart.
Growth and puberty are usually managed by paediatric endocrinologists, who are specially trained paediatricians with an interest in hormone treatment. Fertility issues are usually managed when the young woman has transitioned into the adult endocrine service with a gynaecologist / fertility specialist.
Are there any side-effects to the treatment?
Growth hormone is generally well tolerated but needs to be given daily by injection and can rarely have side-effects such as headaches, visual disturbances, hip or knee pain, and painful or enlarging moles. Growth hormone may also increase the higher risk of type 2 diabetes and lipid disturbances, so girls on growth hormone treatment will be closely monitored.
In low doses, oxandrolone has few side-effects. At higher doses, it can cause abnormal liver function and deepening of the voice, but at usual doses, these are not often a problem.
Although the oral contraceptive pill is widely taken, it does have side-effects in a few individuals such as nausea, vomiting, weight gain, gallstones, high cholesterol, high blood pressure and increased risk of blood clots.
What are the longer-term implications of Turner syndrome?
People with Turner syndrome should be encouraged to lead a healthy lifestyle throughout their life to reduce long-term risks. They should have regular check-ups during adult life, ideally in a specialist Turner syndrome clinic. Adult women with Turner syndrome are more likely to have a number of health issues including high blood pressure, diabetes, and an underactive thyroid gland (hypothyroidism). Repeated ear infections may lead to deafness, if not adequately treated.
Problems with non-verbal skills can give rise to difficulties with arithmetic, constructional tasks, and sense of direction, which could make it harder to learn to drive or read maps.
Whilst unassisted pregnancy is rare, women with Turner syndrome can become pregnant and have babies with IVF using eggs donated from other women. Success with fertility treatment is similar to other cases of ovarian failure.
Further resources:
Turner Syndrome Support Society (UK):