Alternative names for menstrual cycles
Periods; menstrual periods; menstruation
What is the menstrual cycle?
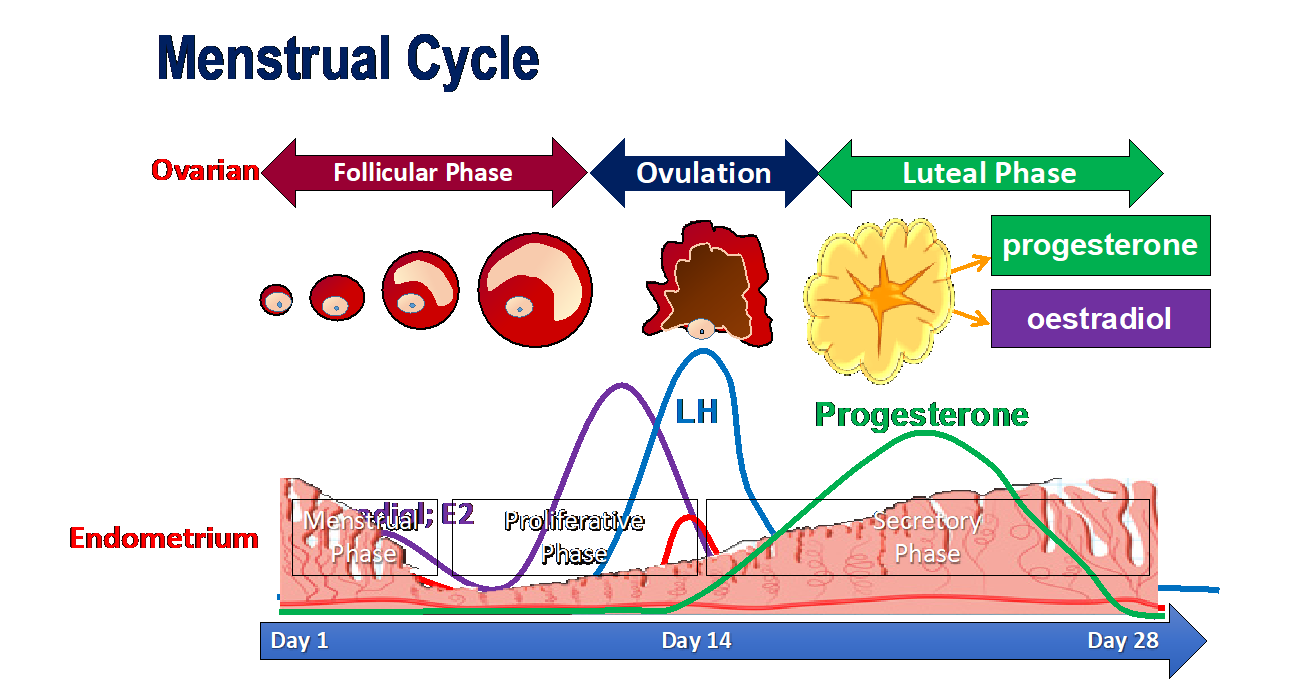
The menstrual cycle is governed by an interaction between reproductive hormones (LH, FSH, oestradiol and progesterone) that result in growth of a follicle (follicles are fluid-filled sacs in the ovaries that contain eggs), ovulation (release of the egg from the ovary into the fallopian tubes), formation of the corpus luteum (remnant of the follicle which produces progesterone and oestrogen to prepare the womb for pregnancy). If no pregnancy occurs, the fall in progesterone leads to shedding of the endometrial (womb) lining and recommencing the cycle. The menstrual cycle typically has a duration of 28 days from the first day of menstrual bleeding until the first day of menstrual bleeding of the next cycle, but can range from 21 to 35 days. Less frequent menstrual cycles are termed ‘oligomenorrhoea’, and absent menstrual cycles are termed ‘amenorrhoea’.
The hormones governing the menstrual cycle change as follows:
- A small rise in follicle stimulating hormone (FSH) occurs at the beginning of the cycle. As the name suggests, this FSH rise stimulates the growth of small follicles (fluid-filled sacs that contain an egg) in the ovary. The first part of the menstrual cycle concerns follicle growth and the selection of a single dominant follicle and is hence referred to as the ‘follicular phase’.
- As the follicles grow, they produce oestradiol and inhibin B. Inhibin B and low levels of oestradiol exert negative feedback on the hypothalamic-pituitary-gonadal axis to reduce FSH levels. This reduction in FSH levels aids selection of the ‘dominant follicle’, because the largest follicles become less dependent on FSH for their continued growth, whereas small follicles perish as they needed sustained FSH exposure. This period, called the ‘FSH window’, leads to selection of a dominant follicle, also known as the ‘Graafian follicle’.
- As the dominant follicle continues to grow, it continues to produce oestradiol. As the oestradiol reaches higher levels, there is a change from negative to positive feedback on the hypothalamic-pituitary-gonadal axis. This leads to a rise in luteinising hormone (LH).
- The mid-cycle rise in LH that last 36-48hrs, leads to ovulation (release of the egg from the follicle) and the remnant of the follicle forms the ‘corpus luteum’. The corpus luteum secretes progesterone and some oestradiol. The maximal rise in progesterone occurs mid-way through the last 14 days of the cycle, termed the ‘luteal phase’. Thus, a raised mid-luteal progesterone is often used to indicate ovulation has occurred.
- The progesterone prepares the endometrium (womb) for implantation in case an egg is fertilised to form an embryo.
- If an embryo forms, it will secrete human chorionic gonadotrophin (hCG) (which can activate LH receptors) to maintain the function of the corpus luteum, such that it can continue to produce progesterone and maintain the pregnancy.
- If no embryo forms and implants, the corpus luteum will no longer survive and this leads to a fall in progesterone.
- The fall in progesterone leads to shedding of the endometrial lining and menstrual bleeding and the cycle recommences.
{kind=link}