Periods
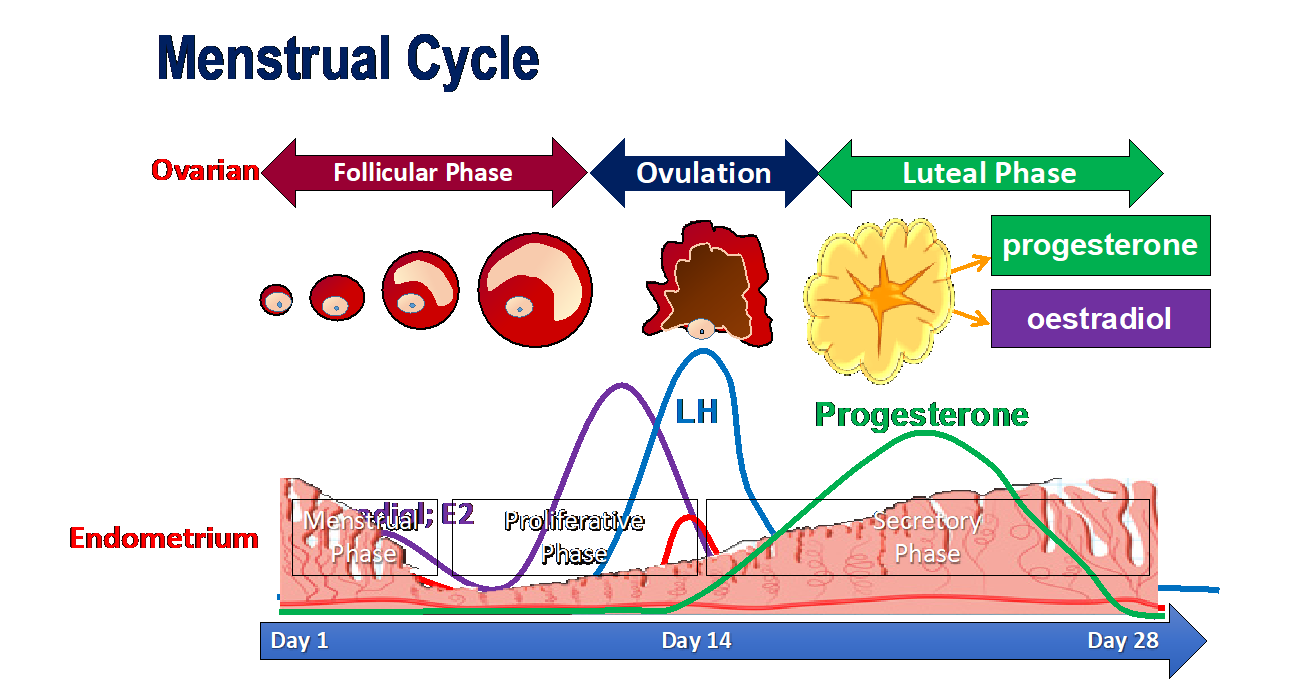
The menstrual cycle is governed by an interaction between reproductive hormones (LH, FSH, oestradiol and progesterone) that result in growth of a follicle (follicles are fluid-filled sacs in the ovaries that contain eggs), ovulation (release of the egg from the ovary into the fallopian tubes), formation of the corpus luteum (remnant of the follicle which produces progesterone and oestrogen to prepare the womb for pregnancy). If no pregnancy occurs, the fall in progesterone leads to shedding of the endometrial (womb) lining and recommencing the cycle. The menstrual cycle typically has a duration of 28 days from the first day of menstrual bleeding until the first day of menstrual bleeding of the next cycle, but can range from 21 to 35 days. Less frequent menstrual cycles are termed ‘oligomenorrhoea’, and absent menstrual cycles are termed ‘amenorrhoea’.
The hormones governing the menstrual cycle change as follows:
Last reviewed: Feb 2021